Beyond the Blood Tests: Why Amyloid PET Remains the Gold Standard
New blood tests may change who gets screened for Alzheimer's and how quickly. The question neurologists are now navigating: when is a blood test enough for diagnosis, and what does this mean for PET imaging?
For many patients, the path to an Alzheimer’s diagnosis begins with a phrase that is more reassuring than diagnostic: “mild cognitive impairment.” As behavioral neurologist Dr. Marwan Sabbagh from the Barrow Neurological Institute explains, “I think doctors don’t know when a person goes from MCI to dementia. Even in the lay audience, people don’t understand that Alzheimer’s is a type of dementia and Alzheimer’s is the type. But I think they use the term MCI because they notice something wrong, and they don’t want to use the boogeyman word of dementia.”
This diagnostic hesitancy has real consequences. Getting the diagnosis wrong has a direct impact on the treatment plan, especially with monoclonal antibody drugs, the first disease-modifying drugs approved for early-stage patients. A rapidly expanding toolkit of blood tests, cerebrospinal fluid (CSF) assays, and gold-standard amyloid PET imaging is giving clinicians more options than ever. The challenge is knowing how they fit together and when amyloid PET remains indispensable.
Fluid biomarkers for screening before imaging
The most significant recent shift in Alzheimer’s diagnostics is the emergence of blood plasma biomarker tests as a practical first step, especially for individuals hesitant about undergoing a lumbar puncture.
These tests measure protein fragments, primarily beta-amyloid 42/40 ratios and phosphorylated tau variants, that diffuse from the brain into the bloodstream. They are minimally invasive, scalable, and increasingly accurate. A June 2025 review in the Journal of Nuclear Medicine frames this well: blood-based biomarkers “hold diagnostic potential together with potentially easy and broad accessibility in the future.” But they provide only indirect, quantitative estimates of amyloid burden and not a direct visualization of what is happening in the brain.
Because anti-amyloid therapies are most effective early in the disease, the ability to confirm diagnosis faster can directly affect patient outcomes. Due to cost and scheduling, it isn’t feasible for everyone who may have Alzheimer’s to undergo amyloid PET imaging. Fluid biomarkers provide an early assessment of risk and act as triage tools.
But the reliability of using blood tests as a standalone confirmatory tool is a topic under debate. Real-world data from Washington University in St. Louis found that roughly 16% of patients who initiated anti-amyloid treatment were confirmed via blood test alone, though this remains the exception. Some primary care doctors and neurologists may be hesitant to use them as standalones. The more common pathway still runs through CSF or PET.
Even the best-performing plasma tests sometimes produce inconsistent results, and according to independent research there may be more variability in their accuracy than manufacturers report, requiring further testing to reach a clinical conclusion. This is precisely where amyloid PET becomes essential.
How blood tests and PET imaging work together
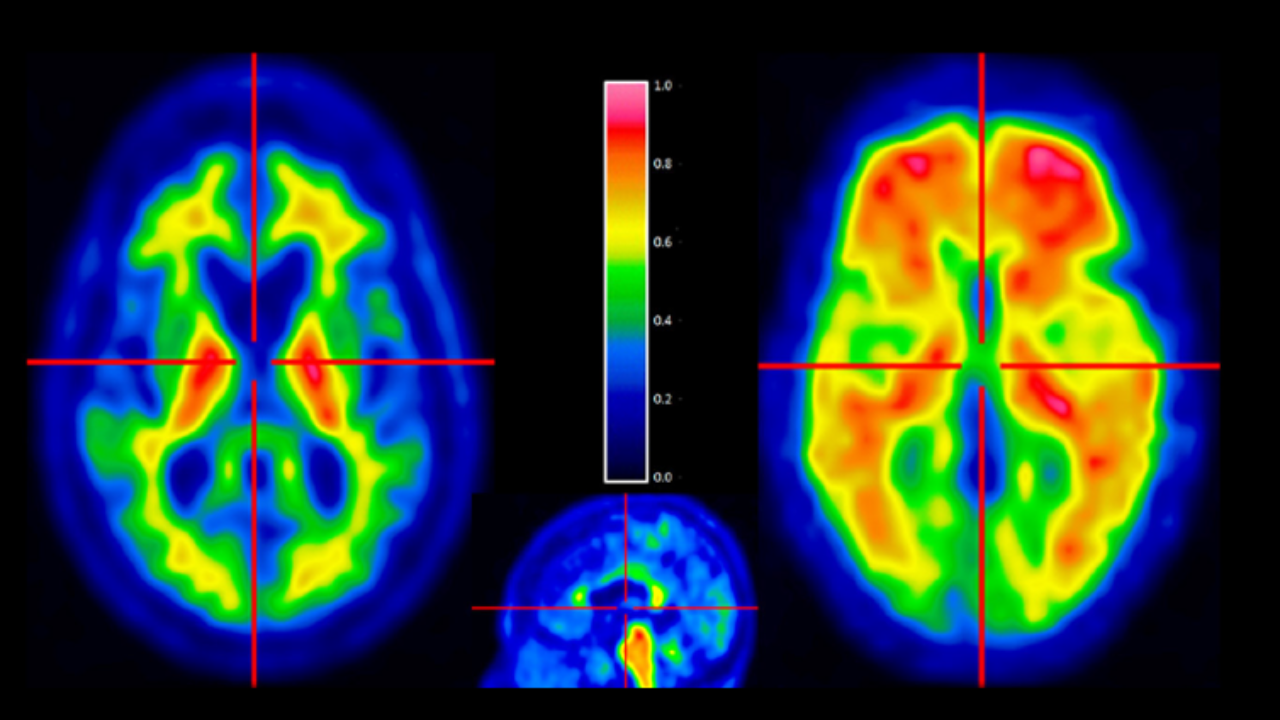
Unlike blood or CSF tests, which measure proxy biomarkers that have diffused out of the brain, amyloid PET provides a direct visualization of amyloid plaque burden across multiple brain regions. Drzezga and colleagues. caution that the risk of clustering biomarker classes together while “neglecting their individual characteristics” leads to “divergent or controversial discussions”, a warning with direct clinical implications for how PET is used relative to blood tests.
Metabolic patterns, distinct across Alzheimer’s, Lewy body and frontotemporal dementia can overlap clinically but diverge on imaging. As Dr. Jacob Dubroff, an associate professor of radiology at the University of Pennsylvania who specializes in molecular imaging for dementia, explains, these are patterns of how the neurons are dying or not using glucose. They are associated with different dementias, but they’re not the same as the amyloid and the tau scans, because those are actually showing the abnormal protein.”
In complex or atypical cases, both types of PET imaging, amyloid and FDG (fluorodeoxyglucose-positron emission tomography), may be needed to reach a confident diagnosis.
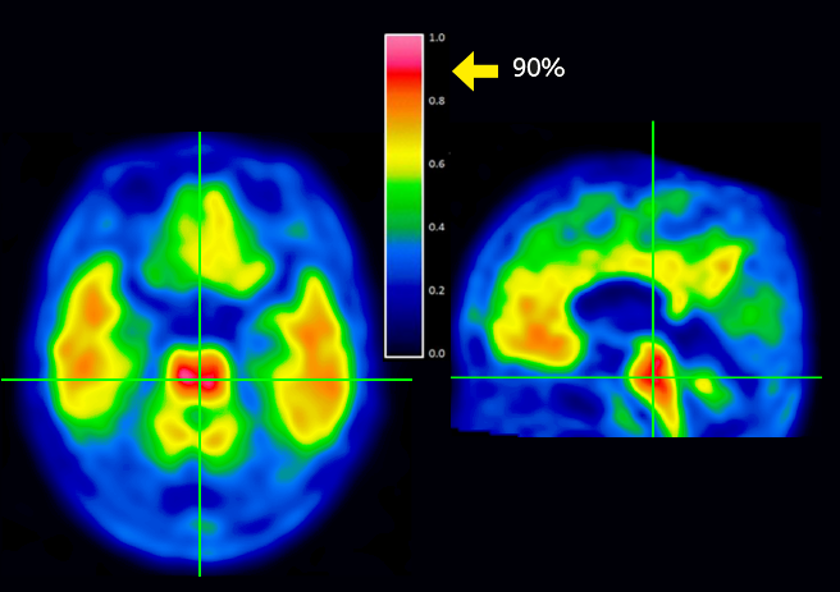
Scan images courtesy of GE HealthCare.
Amyloid PET also has a growing monitoring role beyond diagnosis: tracking plaque reduction is required for patients taking donanemab (Kisunla) to determine when treatment should stop. As more disease-modifying therapies come to market, this function most likely will expand.
Specialists believe that imaging and fluid biomarkers work best as complements, not competitors. Blood tests are ideal for triage, ruling out Alzheimer’s in patients who don’t have it, or flagging those who need confirmatory testing. Amyloid PET remains the gold standard when clinical decisions carry the highest stakes or when determining a specific subtype of dementia.
Dubroff sees blood tests and PET as operating in sequence, not in competition. “The blood test is going to be very good at the outset, helping prioritize who really needs a PET scan,” he told Being Patient. “But once you’re trying to figure out the specific disease and how to treat it, that’s where imaging really becomes essential.”
For neurologists navigating an expanding diagnostic toolkit, his framework is practical: blood tests triage efficiently, but imaging resolves the ambiguity that matters most allowing patients and families to make crucial decisions about their care and future. In the era of disease-modifying therapy, that resolution has direct treatment consequences.








